
 Having any traumatic medical condition is devastating. Humans are constantly evolving and we are learning to deal with different conditions. Several of these conditions can sadly be terminating illnesses. We all know and understand that human life is mortal. Yet, watching a loved one pass away is always very sad. It is hard to accept the truth. Several of the other conditions may not be terminating but equally traumatic. How do we deal with the condition bestowed upon a human? Do we hide it, lie about it or say the truth? There is a science behind lying and how one lie can turn into a thousand lies.
Having any traumatic medical condition is devastating. Humans are constantly evolving and we are learning to deal with different conditions. Several of these conditions can sadly be terminating illnesses. We all know and understand that human life is mortal. Yet, watching a loved one pass away is always very sad. It is hard to accept the truth. Several of the other conditions may not be terminating but equally traumatic. How do we deal with the condition bestowed upon a human? Do we hide it, lie about it or say the truth? There is a science behind lying and how one lie can turn into a thousand lies.
“We often talk about moral values, justice and trust, but the important thing is to put them into effect in our everyday lives.” – Dalai Lama
Ever since growing up as a child, my parents always instilled to say the truth no matter what. While learning US history, the story of honesty as told by George Washington was always highlighted and he went on to become the first US President.Here are some reasons why saying the truth is especially important for people with Androgen Insensitivity Syndrome (AIS) or intersex. Androgen Insensitivity Syndrome (AIS) is a condition that affects sexual development before birth and during puberty. People with this condition are genetically male. They may have female sex characteristics or signs of both male and female sexual development.
1) Honesty is the best policy. Everyone knows this. Not to state the obvious, but saying the truth is in everyone’s best interest. No matter how bitter.
It is best to say the truth for the patient. While having a genetic condition is not in anyone’s control, choosing to lie or say the truth about it is in their control. In the long run, it is best to be truthful. It is better for your heart, mind, and soul. Freedom is an innate human feeling irrespective of gender and by saying the truth, we free ourselves.
2) Truth is what the intersex community is advocating. A first hand account of an intersex person and also community advocacy group want a stop to the concealment-based approach and move to a patient-centric approach when dealing with Androgen Insensitivity Syndrome going forward.
Since the condition was discovered last century, the modus operandi has been a systematic method of secrecy and lying involving the patients, their families, and others. There are several personal stories from first-hand AIS patients where they felt lied to and the lie was actually more devastating than the condition itself. It has long-ranging effects on self-esteem, attitude, psychosocial issues and several other complex issues. Most of these complex issues are issues of the heart or mind and NOT physical like a heart attack or fractured leg. For the surgical treatment in AIS patients, please read further in the article. The point is, it would take a long-term treatment plan to work towards a solution for the psychosocial issues. And whatever the solution, it can only work if based on truth. What good did the institutional and systemic concealment-based approach do for anyone? Clearly, this approach has failed because fundamentally it is based on lies. And anything based on lies does not stand the test of time. It is time to change. Will we ever be able to undo what the lies have already done?
3) Treatment should be truthful. Like any other traumatic medical condition, having an honest diagnosis, prognosis, and treatment plan are essential to the well-being of the humans.
It is well-documented that the treatment plan for AIS patients is part physical where a surgery is needed to remove the male testes and subsequent Hormone Replacement Therapy (HRT). In the best interest of medicine, there should be a feedback mechanism to collect information from the caregivers instead of shutting them out citing privacy. It is a normal practice when treating other traumatic medical conditions where caregivers have more knowledge of the symptoms than the patients. It is also recommended that due to the severe trauma and crisis, and to deal with other psychosexual issues, appropriate therapy be included as part of the treatment plan. Historically, the modus operandi based on the concealment-based approach, is to perform the surgery at a young age and conceal facts from patients and/or family. The family is also “coached” to go along with the concealment in the “best interest” of the patient. The intersex community today is advocating a rethinking to this approach. They want a patient-centric model where the patient decides at an appropriate age whether to have the surgery or not. This questions the medical treatment itself whether the surgery is needed at all to have a fruitful, decent life. Obviously, there are two sides to this debate and too big an issue to get into this article.
If the AIS patient chooses not to have the surgery, then the treatment plan simply is about dealing with the psychological issues and there is no “physical” treatment. And the basis for treatment is simple, the truth! Truth for the patient and truth for all those who love the patient.
4) Truth and support for the caregiver. A caregiver can only be provided the equally needed support if they are allowed to say the truth.
Like any other traumatic medical condition, usually, a family caregiver steps up to care for the loved one. Finding out the truth for the caregiver can be equally traumatic and shocking. The well-documented treatment of this condition is part physical in nature and part psychotherapy. While certainly very traumatic for the patient to find out the truth, is there any trauma for the caregiver who is finding out the truth for the first time? Should the caregiver also be a recipient of the treatment portion of psychotherapy? Or should we call the caregiver a “patient” and that is the ONLY way to get their needs recognized? The only way a caregiver can get the needed treatment and support is if the caregiver is allowed to disclose the truth.
5) Say the truth for a healthy relationship. Like any other relationship, truth is fundamental. Without truth, there is NO relationship.
While the concealment-based approach may have regularized brainwashing, propoganda, falsifying medical records by patients, their loved ones, institutions, systems, it is still not OK in a relationship. Trust is the DNA in a relationship and regardless of the traumatic condition, it is never OK to lie in a relationship. Having this condition is traumatic but putting someone else through it without their knowledge is equally traumatic or worse?
What if the caregiver happens to be the spouse who was not informed about the condition before the marriage. We will not delve into issues such as “same-sex” marriage as it is out of the scope of this article. As you have been educating yourself about AIS, the question must come up at what point does the caregiver become a patient too? Imagine from a spousal caregiver perspective:
a) Just found out the traumatic condition but no help or treatment for the trauma. This not exactly a condition that most people are aware of.
b) Just found out they have been betrayed and lied to.
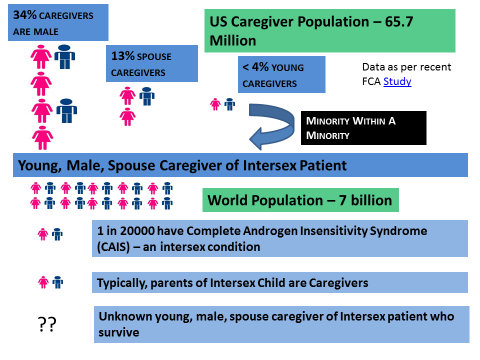
The typical spousal caregiver is a young, male caregiver. Statistically, a minority within a minority. And a young, male, spousal caregiver of AIS is probably countable on your finger-tips out of a population of 7 billion in the world.
6) Truth in the family. A family is a fundamental unit of the society.
As parents, we are always trying for a better life for our children. Even a slight fever is a cause for concern then one can imagine how a parent may feel given this medical condition. Once they have had the chance to recoperate both as a parent and a caregiver, what would be there next steps? Will they choose the traditional, stereotypical path of concealment-based approach or will they rise above and say the truth? After all, as a parent and a caregiver, they would want the best for their child and having an honest, open discussion with the spouse would foster a good life for the AIS child.
7) Truth about the child.
It is a medically accepted fact that AIS patients are infertile. While very unfortunate, today with help of great doctors and medicine, it is possible to have children through Assisted Reproductive Technology (ART). Adoption is also another route and an overwhelmingly preferred route by AIS patients. It would better if counselors would also provide these alternate routes instead of making a blunt and blanket statement to an AIS patient that they cannot be a parent. It has severe, long-term devastating effects and frankly, the counselors are doing more harm than help. And worse, the same counselors will not be around to pick up the pieces when the trauma of their misplaced counseling unravels. In addition to shouldering the responsibility of a caregiver, the young, male, spousal caregiver has been given the additional burden of now convincing the traumatic AIS patient to have a child. Is that fair to the innocent child or the young, inexperienced, unprepared, innocent caregiver? Shouldn’t there be instead support for the caregiver first before increasing their burden? The only way we can provide support and care is by accepting the truth so that everyone’s needs are met. Adoption is a preferred approach of AIS patients to have kids. There is so much regulation involved when adopting. Why is there NO regulation provided to the caregiver when making the same choice at a young, inexperienced, vulnerable stage in wanting to have a biological child?
8) Truth for the child.
Human beings like to procreate. It is a very natural feeling. Like any expert parenting resources will state that taking care of an infant is both very nurturing and takes time and patience. It is well-documented both medically and first-hand accounts of AIS patients that knowing the truth and the subsequent surgery (if elected) is very traumatic and patient is in a crisis. How then can a person struggling through their own personal trauma and crisis be able to take care of an infant requiring patience and nurturing? Physically, an AIS patient gets on Hormone Replacement Therapy (HRT) after surgery to remove testes. What are the effects of this HRT physically in the body, mind, emotions? Will they be able to care for an infant at the same time? Are there any medical studies to evaluate a waiting period? Because this situation is so rare and never talked about does not mean it does not occur. Does the medical community have enough scientific data and/or the interest in pursuing a research study?
How would it be for the caregiver at the same time to see a loved one go through this heights and valleys in emotions and the resulting actions. Do you forgive the insulting actions or leave as a caregiver? How does a caregiver balance between the emotions of caring for a loved one, a spouse Vs. caring for their own biological new born child? Is the caregiver in a double whammy situation? These are areas probably hardly ever been visited before from a young, male, spousal caregiver perspective.
It is a brave and honest person who can stand apart from the masses and openly challenge its most treasured beliefs. ~ Donna Evans
And most importantly, what is in the best interest of the child? If the truth were allowed to be said, the caregiver would have more support, the patient would have more support and ultimately, the innocent child would have a better life. In rushing to caring for the patient, have we forgotten about an innocent infant life?



 Facebook
Facebook GooglePlus
GooglePlus RSS
RSS Twitter
Twitter